
As sports physiotherapists we readily prescribe exercise programs to our athletes/patients – quite simply – it is a massive part of what we do. As well as exercises, we also tell our patients what they should NOT be doing – “You should not do this OR that”! Have you ever wondered how much they really take our advice? Unfortunately (for both us and the patient) our patients are frequently non-compliant with our rehabilitation programs.So here are some evidence based tips to improve patient compliance!
Cervical radiculopathy is a pathology of the cervical nerve root (Dox et al 1979), frequently associated with cervical disc herniation or another space occupying lesion (such as osteophytes), which can cause nerve root impingement and inflammation. As many of you will be aware, this can be a very painful and often debilitating condition. Although the natural history of the condition is favourable, it has been suggested that if the condition becomes chronic it can be recurring and impact negatively on physical and mental health. Therefore, it is essential that as physiotherapists we are aware of the most evidence informed diagnosis and treatment techniques for cervical radiculopathy.
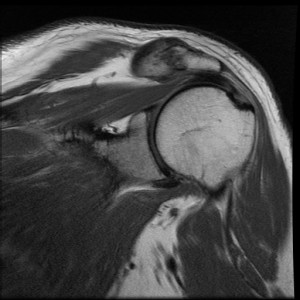
Acromioclavicular injuries are common in a variety of sports, particularly those which involve heavy contact or tackling. For example, Flik et al (2005) reported the incidence of AC injuries was the third most common in men’s ice hockey. Thus, this is a common injury. Whilst in many injury cases, such as acute presentations and the higher grade AC separations, the diagnosis can be quite obvious. However, many conditions of the shoulder present with very similar clinical presentations, and thus differential diagnosis can be challenging (Meyer et al 1990). Thus, this article examines the diagnostic accuracy for clinical examination tests for acromioclavicular joint pain.
INTRODUCTION Many of you, I’m sure, will be interested to learn to efficacy of PRP injections for treating athletes with chronic achilles tendinopathies. PRP has gained significant attention of late; in the media, medical community and with our athletes. It seems my athletes are always asking for information on the most effective form of injectional […]
Plantar heel pain, or commonly plantar fasciitis, is a very common clinical presentation. In an athletic population of runners, plantar heel pain has been shown to account for as much as 8% of injuries (Taunton et al 2002). Thus, sports physiotherapists should be aware of the most appropriate management techniques for this condition. Recently support for the effectiveness of myofascial trigger point therapy has come from a randomised controlled trial. The results and techniques utilised in the trial are discussed in this post.

Neck pain is a common clinical presentation, affecting up to two-thirds of the population at some time in their life. Therefore, as sports physiotherapists we will regularly assess and treat athletes with recent onset neck pain. As a component of rehabilitation many physiotherapists will include some form of evidence based manual therapy, commonly either mobilisation or manipulation. However, a clinical question I am often asked (by both myself and patients) is what additional benefits does manipulation provide, given the additional risks? This clinical question is answered by a recent RCT that compares the use of mobilisation and manipulation in patients with recent onset neck pain.