
Introduction
A muscle haematoma, or “cork” as they are often called, is a common occurrence in many sports. These muscles haematomas are most prevalent in those who participate in contact sports; such as rugby and football (Smith et al., 2006). Quite obviously, this is something that sports physiotherapists will commonly encounter, particularly those involved with the aforementioned sports. This article discusses the evidence based management (well…the best available evidence) for muscle haematomas.
Definition and Mechanism of Haematoma
A haematoma is a local accumulation of blood in a tissue, space or organ. In muscle it has 2 mechanisms of injury (Klein et al, 1990):
- Direct: following direct impact or contusion
- Indirect: following a tear or rupture of fibres of the muscle
Types of Haematoma
There are two types of muscular haematoma:
Intramuscular Haematoma: in an intramuscular haematoma the muscle sheath and the fascia will remain intact. This will have the effect of confining the bleed within the tissues (this increased pressure has the potential to compress capillary beds and counteract the bleed) (Bird et al., 1997). This effectively means that signs and symptoms will remain localised. It’s characteristics include:
- Swelling (beyond 48 hours). This is because the contained blood causes an osmotic gradient and interstitial fluid is drawn into the muscle (Peterson and Renstrom, 2001).
- Pain and tenderness
- Decreased muscle function (reduced contraction and extensibility)
Inter-muscular Haematoma: In this case the fasica/sheath is torn. This allows communication of the fluid between muscles/compartments. This leads to dramatic bruising and swelling which travels distally secondary to gravity. Generally in the case of inter-muscular haematomas the pain settles considerably following the first 24 hours (Smith et al., 2006).
Physiotherapy Treatment of Muscle Haematoma
As sports physiotherapists we have quite a few tools in our toolbox that we could hypothetically aim at a muscle haematoma. Smith et al. (2006) performed a review of the literature to identify which of the following treatments, which are regularly advocated for the treatment of muscle haematoma/corks, have any evidence base. This is a summary of what they found:
Acute Phase Management (First 24 – 72 hours)
REST: It is important that the athlete undergo a period of relative rest. Whilst the athlete should not ignore the pain, once the athlete can move the limb they should do so (Renstrom, 2003). Early mobilisation is widely advocated (Smith et al., 1996).
ICE: has been proposed in the acute stages due to its physiological effects on blood vessels i.e. vasoconstriction. Ice is proposed to reduce:
- Blood Flow
- Oedema
- Muscle Spasm
- Metabolism (and therefore secondary hypoxic damage)
- Pain
- Muscle Inhibition
Whilst multiple animal studies have been performed (which frequently present contradictory findings) there is undoubtedly widespread anecdotal evidence for its use following acute injuries. As I have previously discussed on this blog, the application of ice has yet to be research backed guidelines on application time and method (Bleakely et al., 2004).
COMPRESSION: No conclusive evidence can be drawn on the effectiveness of compression. However, the physiological effects are undeniable. Thorsson et al. (1987) showed moderate compression was able to reduce intramuscular blood flow by up to 50% in healthy athletes.
ELEVATION: Again, no conclusive evidence can be drawn from the studies, however, there are the physiological effects of decreased arterial pressure and increased venous return. The application of which is obvious in haematoma management.

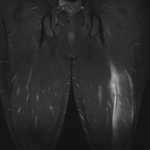
Muscle Haematoma Injury
Resolution Phase Management (72 hours +)
HEAT: Giombini et al. (2001) showed that hyperthermia was superior to ultrasound therapy for reduction of VAS and haematoma resolution following lower limb sports injuries. Such an improvement in haematoma resolution was mirrored by animal studies performed Lehmann et al. (1983).
ULTRASOUND: There are some studies that examined the effects of ultrasound following muscle haematoma and their effects on haematoma absorption, however, they present conflicting results. Some studies have shown increases in cellular activity (of unknown statistical significance),whilst others do not. Additionally, it is also possible that the positive effects reported by some studies are a result of the thermal effects of ultrasound. Thus, it is challenging to draw clear conclusions of the role of ultrasound in muscle haematoma management.
EXERCISE: In this phase AROM and isometric exercises are widely advocated (Smith et al., 2006). This is generally progressed to include resistance exercise (see table below).
COMBINED PROGRAMS: There have been a few studies that have studies the use of a “Combined Program” which has included a 3 phase program (Smith et al., 1996; Ryan et al., 1991). However, it is challenging to draw any conclusions on the effectiveness of the programs as none include a control or non-intervention arm. The table below discusses the overall components of the combined programs.

Muscle Haematoma Combined Treatment Program (Smith et al., 2006)
No Evidence
There was no evidence/studies which examined the role of the following treatments. Additionally, they were not commonly proposed by a variety of sports medicine textbooks (Smith et al., 2006):
- Thermal Contrasts
- Massage
- Electrical Stimulation
Whilst it is clear that these modalities may have theoretical and/or physiological applications following a haematoma injury, they have not been studies or widely advocated.
Myositis Ossificans
Myositis ossificans is a serious and relatively common (~10%) complication following muscle haematomas (Smith et al., 2006). It has the following characteristics:
- Radiologically evident after 3 – 6 weeks
- Significant loss of ROM
- Significant tenderness and hardening on palpation
- More common in intramuscular haematomas
In the presence of myositis ossificans rehabilitation should include:
- Rest
- Gentle Rehabilitation
Prognosis
There have been a wide range of recovery periods following muscle haematoma. Intramuscular haematomas have a worse prognosis than intermuscular haematomas (Smith et al., 2006). Other poor diagnostic indicators include reduced distal pulses and paraesthesias.
Ryan et al. (1991) evaluated the use of combined program (see above) following quadriceps contusions and found the following results. The average time to recovery was
- Mild Injuries (knee ROM at 12 0 24hrs > 90 degrees): 13 days
- Moderate Injuries (knee ROM at 12 0 24hrs 45 – 90 degrees): 19 days
- Severe Injuries (knee ROM at 12 0 24hrs < 45 degrees): 21 days
Take Home Messages
- There are 2 mechanisms (direct and indirect)
- There are 2 types of muscle haemotoma (intramuscular and inter-muscular)
- Intramuscular haematomas have a worse prognosis than inter-muscular
- Acute Phase = RICE
- Resolution Phase = Heat, Exercise (and possibly US)
- Sport Specific Phase = Increasing Resistance Exercise
- Beware of Myositis Ossifican
What are your thoughts?
What is your experience with the treatment of muscle haematomas and corks? Be sure to let me know in the comments or catch me on Facebook or Twitter
If you require any sports physiotherapy products be sure check out PhysioSupplies (AUS) or MedEx Supply (Worldwide)
Photo: Ed Yourdon , Monica’s Dad
References
Bird S, Black N, & Newton P. (1997). Sport injuries. Causes, diagnosis, treatment and prevention. Cheltenham, UK: Stanley Thornes Ltd.
Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sport Med. 2004; 32:251–261.
Giombini A, Casciello G, Di Cesare MC, Di Cesare A, Dragoni S, & Sorrenti D. A controlled study on the effects of hyperthermia at 434MHz and conventional ultrasound upon muscle injuries in sport. Journal of Sports Medicine and Physical Fitness 2001;41:521–527.
Klein JH. Muscular hematomas: Diagnosis and management. Journal of Manipulative Physiology and Therapeutics 1990 13:96–100.
Lehmann JF, Dundore DE, Esselman PC, Nelp WB. Microwave diathermy: Effects on experimental muscle hematoma resolution. Archives in Physical Medicine and Rehabilitation 1983;64:127–129.
Peterson L & Renstrom P. (2001). Sports injuries. Their prevention and treatment (3rd ed.). London: Martin Dunitz.
Renstrom P. (2003). Muscle injuries. In J. Ekstrand, J. Karlsson, & A. Hodson (Eds.), Football medicine (pp. 217–228). London: Martin Dunitz.
Ryan JB, Wheeler JH, Hopkinson WJ, Arciero RA, & Kolakowski KR. Quadriceps contusions. West point update. American Journal of Sports Medicine 1991: 19, 299–303.
Smith TO, Hunt NJ, Wood SJ. The physiotherapy management of muscle haematomas. Physical Therapy in Sport 2006 7(4): 201-209
Thorsson O, Hemdal B, Lilja B, Westlin N. The effect of external pressure on intra-muscular blood flow at rest and after running. Scandinavian Journal of Medicine and Science in Sports. 1987; 19:469–473.
Related Posts
 Comparing 2 Rehabilitation Programs for Hamstring Injuries
Comparing 2 Rehabilitation Programs for Hamstring Injuries Facilitating VMO Activation with Isometric Hip Adduction
Facilitating VMO Activation with Isometric Hip Adduction How Mechanism of Injury Affects Prognosis Following Hamstring Strain
How Mechanism of Injury Affects Prognosis Following Hamstring Strain Thoracic Outlet Syndrome: Assessment and Management
Thoracic Outlet Syndrome: Assessment and Management Lumbar Spine Mobilisation For Hamstring Strains
Lumbar Spine Mobilisation For Hamstring Strains What Arnold Schwarzenegger Taught Me About Scapular Rehabilitation
What Arnold Schwarzenegger Taught Me About Scapular Rehabilitation
Comments
Physiotherapy in Kolkata
Hi,
I wanted to use this blog to share with you my wonderful experience in Physiotherapy. I am a working IT professional and have to sit long hours in front of the computer due to which I had excessive neck and shoulder pain. I was not sure what to do as the pain was becoming unbearable and my work was suffering. I had the opportunity to meet Dr. Hironmoy Sil and he helped me a lot with my physiotherapeutic problems. He counseled me, corrected my sitting posture, working method so that I can continue with my long hours in work. He asked me to do some regular exercise and change my sitting posture. Slowly and steadily we had quite a few sessions and I was highly relieved with the results.
I want to share this with all my IT and ITES friends who are constantly having this pain and are unable to work properly. Dr. Sil has been extremely cooperative and has taken physiotherapy to the next level. Based in Kolkata he counsels the patients and works with them to help them overcome the professional stress, injury, orthopedic problems by helping them with the right physiotherapy treatment.
I would highly recommend Dr. Hironmoy Sil. For further information you can visit his website http://www.hironmoysil.com .
Thanks
Interesting read, needed info following injury
I have a gluteal intramuscular hematoma not due to injury but due to an IM injection of morphine. They did an ultrasound to diagnose and suggested to just watch it and ice it. Now 2 days later it is even more swollen and painful. I am not sure what to be looking out for and how long it will continue to get worse before it improves. If there is a point that I should be going back to the doctor. There is no discoloration on the skin but it was not externally traumatized. The hematoma is underneath the muscle. What do you suggest?
iam a sports physiotherapist and working as assisstant professor. this website is really good and useful
I fell in my yard on a large granite rock about a week ago. I developed a large hematoma on my right calf near the front of my tibia. I iced it initially which did reduce edma. Theis about 4 inches long by 3 inches wide. It does not seem to be getting better after a week and the blood is following down by the side of my ankle. In November I had nerve decompression surgery in the same area of mr ankle and now experiencing pain in the area of the ankle and an increase of neuropathy in that area. The hematoma is quite hard and the pain is increasing and it is difficult to walk. I also now have pain in the ankle when I walk. I’m reluctant to seek medical treatment because I am scheduled to have surgical ERCP tendon repair on Thursday and don’t wish to postpone that surgery due to my insurance carrier changing shortly and neither the hospital or surgeon in NYC will accept Blue Cross Blue Shield. It’s a Catch 22 situation that and I do not want to create a permeate situation by waiting another week or so until after my shoulder surgery. Any practicle advice out there? I am in pain, but my elbow is my main concern. I don’t want to make a mistake and end up with worse problems………Thanks for any advice!
Hi I’m radiologist medical and I’m stadi trauma to the Footboll players . I’m interesting about hematoma and the ather trauma muscular rupture .